


1Dermatology and Venereology Unit, Department of Medicine Solna, Karolinska Institutet, 2Department of Dermatology, Karolinska University Hospital Solna, 3Dermatological and Venereal Clinic, Södersjukhuset, 4Department of Public Health Sciences, Karolinska Institutet, and 5Centre for Epidemiology and Community Medicine, Stockholm County Council, Stockholm, Sweden
The associations between atopic dermatitis (AD) and cardiovascular disease (CVD) are debated. The aim of this study was to investigate the association between AD and coronary artery disease or ischaemic stroke in a nationwide, register-based, case-control study (104,832 AD cases, 1,022,435 controls) based on linkage of Swedish national register data between 1968 and 2016. Patients were classified as having severe AD if they had received systemic pharmacotherapy for AD or had been treated in a dermatological ward with AD as the main diagnosis. Other AD was classified as non-severe. After multivariable adjustments for comorbidities and socioeconomic status, overall AD was associated with angina pectoris (adjusted odds ratio (aOR) 1.13, 95% confidence interval (CI) 1.08–1.19), but among males with severe AD this association was not found, compared with the general population. Male non-severe AD was associated with myocardial infarction (OR 1.15, 95% CI 1.07–1.23). Severe AD was associated with ischaemic stroke, with similar estimates in men and women (aOR 1.19, 95% CI 1.07–1.33). Subgroup analyses among women indicated smoking as an important risk factor among severe cases. Dia-betes mellitus, hyperlipidaemia, and hypertension were more prevalent in severe AD than in controls, and hyper-lipidaemia and hypertension were also more prevalent in non-severe AD than in controls. In conclusion, in this study, AD was associated with CVD, and this should be kept in mind, especially when managing patients with severe AD.
Key words: angina pectoris; atopic dermatitis; coronary artery disease; comorbidity, eczema; myocardial infarction; stroke.
Accepted Jun 13, 2019; E-published Jun 14, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Lina U. Ivert, Department of Dermatology, Karolinska University Hospital Solna, SE-171 76 Stockholm, Sweden. E-mail: Lina.ivert@ki.se
Studies show conflicting results regarding the association between atopic dermatitis and cardiovascular disease. The aim of this study was to investigate the association between atopic dermatitis and angina pectoris, myocardial infarction, or ischaemic stroke in a nationwide, register-based, case-control study among Swedish patients aged 15 years or older. Adult patients with atopic dermatitis were found to have a positive association with angina pectoris, myocardial infarction, and ischaemic stroke, compared with the general population. The association between atopic dermatitis and cardiovascular disease was attenuated after adjustment for cardiovascular comorbidities and education.
Atopic dermatitis (AD) is a common chronic inflammatory skin disorder with a lifetime prevalence of 10–20% in developed countries (1, 2). The pathogenesis of AD is complex, with interactions of multiple genetic, biological and environmental factors leading to skin barrier dysfunction and altered immunological response. AD can have a severely negative impact on health-related quality of life, including self-confidence and sleep, and it also implies a socioeconomic burden, with loss of working days and extensive use of healthcare resources (3).
Associations between AD and atopic comorbidities, such as asthma, allergic rhinitis, and food allergies, are well-established (1). In recent years, several studies have explored associations between AD and non-atopic comorbidities; for example, cardiovascular disease. It has been suggested that the chronic systemic inflammation in patients with AD may trigger arteriosclerosis and cardiovascular disease, in line with the observed risks among patients with psoriasis (4, 5). However, a meta-analysis using adjusted effect estimates reported no association between AD and myocardial infarction, hypertension, diabetes mellitus, or stroke, although a modest association with angina pectoris was found. The authors concluded that variations in risk factors, such as obesity and smoking, might explain positive associations in different populations, and that AD is unlikely to represent an independent risk factor for cardiometabolic disease (6). On the other hand, most of the studies included were cross-sectional and, in some, the AD diagnosis was based on questionnaires not specific for AD. Furthermore, in a large population-based study from the UK, patients with severe AD had a significantly higher risk of stroke and cardiac outcomes (7). Also, a recent systematic review and meta-analysis found that significant associations between AD and cardiovascular outcomes were more common in cohort studies, but with between-study heterogeneity, and that increasing AD severity was associated with cardiovascular outcomes (8). Thus, in summary, epidemiological studies have shown conflicting results.
The aims of this study, using well-established nationwide Swedish healthcare registries, were to assess the association between AD at age 15 years or older and coronary artery diseases (CAD; i.e. angina pectoris and myocardial infarction (MI)) or ischaemic stroke, and to determine whether the magnitude of any such associations varied with severity of AD.
A nationwide, register-based, case-control study was conducted based on linkage of Swedish national register data between 1968 and 2016 to assess cardiovascular (CVD) comorbidity and mortality among patients with AD. The source population comprised Swedish patients aged 15 years or older between the years 1968 and 2016. All patients with an inpatient diagnosis of AD (from 1968) or an outpatient diagnosis of AD (from 2001) through 2015 were included in the study population. The use of the unique personal identification numbers assigned to all individuals living in Sweden allowed record linkage to several national registers, as described below.
AD was defined in accordance with the International Classification of Diseases (ICD) (ICD-8 between 1968 and 1986: 691, ICD-9 between 1987 and 1996: 691, and ICD-10 from 1997: L20.0–L20.9). The National Patient Register (NPR), which includes information on inpatient care from 1964 and outpatient, non-primary care from 2001, was used to identify suitable patients. Patients were classified as having severe AD if they had received systemic pharmacotherapy for AD (methotrexate, azathioprine, cyclosporine, and/or mycophenolate mofetil) or if they had been treated in a dermatological ward with AD as their main diagnosis. Other AD was classified as non-severe. Exclusion criteria for the AD cases were reused IDs and/or persons with incomplete records.
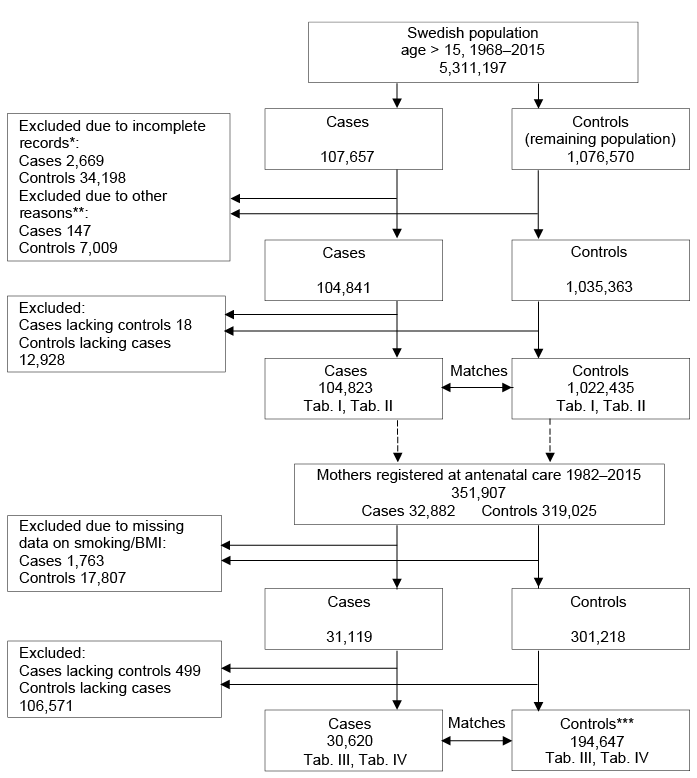
For comparison, 10 randomly selected age- and sex-matched control subjects were identified from the Total Population Register (TPR) for each case of AD. Some controls did not have complete records and the pregnancy criterion resulted in a major reduction in participants in the subgroup analysis (Fig. 1). Therefore, the control-to-case ratio was increased to 10:1 in order to obtain a ratio of approximately 5:1 in the final analysis. Exclusion criteria for the controls were: reused IDs, persons with incomplete records, and AD diagnosis before age 15 years. Information on dispensed drugs was collected from the Swedish Prescribed Drug Register (data available from July 2005). The comorbidities CAD and ischaemic stroke were identified using ICD codes from NPR and the Swedish Death Register (see Table SI for ICD codes used). The data was used in the linkage between registries.
Fig. 1. Study flow chart. *Mainly missing education level. **Reused personal numbers, controls with atopic dermatitis (AD) before age 15 years. ***The pregnancy criterion resulted in a major reduction of participants. Controls had to be pregnant during the period of interest and they also had to be matched to a case that had been pregnant during the period of interest. BMI: body mass index.
The highest attained level of education was included as a proxy for socioeconomic status and obtained from the Longitudinal Integrated Database for Health Insurance and Labour Market Studies (LISA) (9).
Education was categorized into 3 groups: ≤ 9, 10–12 and > 12 years of education.
Data on smoking and body mass index (BMI) were available from the Medical Birth Register (MBR) for the subgroup of women registered for antenatal care between 1982 and 2015. Light smoking was defined as 1–9 cigarettes/day and heavy smoking as ≥ 10 cigarettes/day. BMI was categorized as underweight (< 18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2) or obese (≥ 30 kg/m2). For mothers with more than one child and multiple registrations in MBR, data on the highest number of cigarettes/day and the highest BMI were included.
In accordance with the ICD classifications, patients were classified as having diabetes mellitus if they were treated with insulin or oral hypoglycaemic agents, or had documented hyperglycaemia with dietary restrictions.
Statistics Sweden (SCB) maintains the TPR and LISA, while the National Board of Health and Welfare maintains the other registers used in this study.
Conditional logistic regression was conducted to calculate sex- and age-adjusted crude and adjusted odds ratios (OR) with 95% CI as estimates of the association between AD and CAD or ischaemic stroke in relation to controls. Multivariate models were adjusted for comorbidities (diabetes mellitus, hyperlipidaemia, hypertension) and education level. Stratified analyses and visually evaluated effect modifications were conducted. We did not find any such association for the comorbidities diabetes mellitus, hyperlipidaemia, or hypertension. For associations between AD and CVD, each covariate was included (diabetes mellitus, hyperlipidaemia, hypertension, smoking, BMI, and education) separately, to test for confounding. The adjusted estimates differed from the crude estimates by >10% for hypertension and smoking, but not for education, diabetes mellitus, hyperlipidaemia, or BMI. In line with previous studies, education, diabetes mellitus, hyperlipidaemia, and hypertension were included in the final adjustment model. Smoking and BMI were also added for a subgroup of women in secondary multivariate models. Outcomes and covariates were compared between cases/controls using Pearson’s χ2 test and Student’s t-test for independent samples. Emigration, where people who have moved abroad could get a cardiovascular disease without us knowing, did not change the result. The analyses were not adjusted for multiple hypothesis testing (10) and were conducted using SPSS, version 20 (IBM, Armonk, NY, USA).
The study was approved by the Regional Ethics Review Board, Stockholm (2016/2496-31). All data were anonymized before analysis.
In total, 107,657 patients with AD were identified. After applying the exclusion criteria, 104,823 patients with AD and 1,022,435 matching controls remained, as shown in the flow chart (Fig. 1). The characteristics of the cases and the matched controls are shown in Table I. Most cases were identified as non-severe (95,274; 91%). There was a female predominance among both non-severe (66.2%) and severe (64.3%) cases of AD.
Table I. Characteristics of the study population. Patients with atopic dermatitis divided into severe cases and non-severe cases
The associations between AD and CAD or ischaemic stroke are presented in Table II. In the primary analysis, there were significant associations between AD and angina pectoris (OR 1.18, 95% CI 1.13–1.23), MI (OR 1.10, 95% CI 1.04–1.15), and ischaemic stroke (OR 1.07, 95% CI 1.02–1.13). These associations decreased in the adjusted model: angina pectoris (aOR 1.13, 95% CI 1.08–1.19), MI (aOR 1.07, 95% CI 1.02–1.12), and ischaemic stroke (aOR 1.04, 95% CI 0.99–1.09).
Table II. Risk of coronary artery disease and stroke in patients with atopic dermatitis (AD) compared with individuals without AD
Mean age at first ischaemic stroke or at death from ischaemic stroke was lower in patients with AD than in controls (severe cases: 67.1 vs. 68.5 years, p = 0.048; non-severe cases: 66.1 vs. 67.2 years, p = 0.013; Table I), but not age at first MI or at death from MI. AD was not associated with death from MI or ischaemic stroke.
After multivariate adjustments, a positive association was found between non-severe AD and angina pectoris (aOR 1.13, 95% CI 1.08–1.19), and after stratification by sex this association persisted in both sexes (Table II). The association between non-severe cases and MI remained consistent for men (aOR 1.15, 95% Cl 1.07–1.23), but not for women. Non-severe AD was not significantly associated with ischaemic stroke.
Individuals with severe AD had significantly higher prevalence of diabetes mellitus (7.9% vs. 6.3%, p < 0.001), hyperlipidaemia (6.0% vs. 5.0%, p < 0.001), and hypertension (21.0% vs. 16.4%, p < 0.001) compared with controls (Table I). After multivariate adjustments and stratification for sex, the higher ORs for angina pectoris (aOR 1.11, 95% CI 1.00–1.24) persisted only among women (aOR 1.19, 95% CI 1.04–1.37) (Table II). There was no significant association with MI. Patients with severe AD had a significant association with ischaemic stroke (aOR 1.19, 95% CI 1.07–1.33), which remained after adjustment in both men and women.
There was no significant association between patients on systemic treatment and CVD in adjusted models.
Mothers with severe AD had a significantly lower level of education and higher prevalence of smoking (28.2% vs. 19.9%, p < 0.001) and obesity (12.0% vs. 9.6%, p < 0.001) than controls (Table III). Notably, mothers with non-severe AD smoked less and had less overweight than control subjects. The association between AD and angina pectoris remained for severe cases in the fully adjusted model (adjusted for comorbidity, education, smoking, and BMI) (aOR 1.51, 95% CI 1.00–2.28) (Table IV). There was no significant association between AD and MI or ischaemic stroke in the fully adjusted models.
Table III. Characteristics of mothers registred at antenatal care 1982–2015. Patients with atopic dermatitis divided into severe cases and non-severe cases
Table IV. Risk of cardiovascular disease among mothers with atopic dermatitis (AD) registred at antenatal care 1982–2015 compared with individuals without AD
This large, nationwide study using well-established Swedish healthcare registries and unique personal identification numbers, investigated the association between AD and CVD. The main findings were that patients with AD in Sweden had a positive association with angina pectoris, MI, and ischaemic stroke, compared with the general population. No association was found with cardiovascular death. The association was attenuated after adjustment for cardiovascular comorbidities and education. Subgroups with higher ORs for CVD were identified after stratification for sex and severity of AD. Overall, there was an association with angina pectoris after multivariable adjustment, but not among males with severe AD. Being male with non-severe AD was associated with having MI, but this association was not seen in the severe AD group or in females. Furthermore, severe AD was associated with ischaemic stroke, with comparable rates in men and women.
Information on common cardiovascular risk factors, such as smoking and obesity, was not available for the entire study population. However, the prevalence of smoking and obesity were investigated by analysing women registered in antenatal care, used as a proxy for postpartum smoking and obesity (11, 12). When controlling for smoking, education, comorbidities and BMI in the subanalysis of mothers, the association between angina pectoris/stroke and severe AD decreased (e.g. from OR 2.2 to OR 1.51). Additional adjustment for BMI changed the estimates only slightly. Notably, adjusting for smoking and BMI did not affect the overall analysis and estimates among non-severe cases. This may indicate that smoking is an important confounding factor among cases with severe AD, but not among non-severe cases or in the overall analyses. Since the women registered in antenatal care were younger than the study population, the estimates for the association between AD and CAD or ischaemic stroke cannot be generalized.
Several factors may contribute to an increased risk of CVD. In meta-analyses, there are associations between AD and obesity/smoking which per se increase the CVD risk (13, 14). Smoking, drinking alcohol, sedentary lifestyle, and sleep deprivation are reported to be more common in adults with AD (15). Several biomarkers in peripheral blood correlate with AD activity and cytokine activation, suggesting a systemic disease (16). Chronic diseases seem to lead to overexpression of T-helper 1 (Th1) cell-mediated cytokines (which are involved in arteriosclerosis) and increased Th17 cell-mediated responses (17, 18). This may explain the higher association with CAD and ischaemic stroke among severe and chronic cases of AD, while non-severe AD was not associated with stroke. It remains unclear whether AD is an independent risk factor for CVD or if reported associations can be explained by established cardiovascular risk factors, lifestyle or other factors, such as systemic immunosuppressive therapy (19). In the adjusted models in our study, we did not find higher ORs between severe AD treated with systemic therapy and CVD, but this group did have a higher prevalence of cardiovascular comorbidity. Diabetes mellitus, hyperlipidaemia, and hypertension were more prevalent in severe AD than in controls, and hyperlipidaemia and hypertension were also more prevalent in non-severe AD than in controls.
The current finding that AD is correlated with angina pectoris is in agreement with previous studies (6, 20). However, in a meta-analysis, there was no significant association between AD and MI (6). In a recent large cohort study, severe AD increased the risk of MI and angina pectoris by 40–50% (7). The risk of MI is approximately 3 times higher in men than women in the general population. The incidence becomes more similar with increasing age, especially among women with risk factors such as smoking, diabetes mellitus, or hypertension (21). This may partly explain why we found that AD was associated with MI in men only.
In accordance with large population-based studies from the UK and Taiwan, it was found that severe AD might be a risk factor for stroke (7, 22), while cohort studies from Denmark and Germany could not confirm this association in adjusted models (20, 23). Only in the study from the UK were lifestyle factors, such as smoking and BMI, included in the fully adjusted analysis. AD was not independently associated with non-fatal MI or stroke in a female cohort of nurses in The Nurses’ Health Study in the USA (24). Nurses are, in general, likely to be more health-orientated (25). In comparison, the current subgroup of women with severe AD had a higher prevalence of smoking, BMI, and lower level of education. Differences in study populations and study designs, observation periods, definitions of AD (e.g. questionnaire-based diagnosis or diagnosis by general practitioners or by dermatologists) and whether stratification by AD severity was performed most likely explain the mixed findings between the previous studies.
The strengths of the current study are the use of a nationwide large population-based cohort and high-quality inpatient and outpatient data linked to several national registers, together with the use of the unique personal identification numbers given to all Swedish residents. The large sample size gave substantial statistical power and allowed examination of AD subgroups. A major strength is that, in 93% of severe and 79% of non-severe cases of AD, the diagnosis was confirmed by a dermatologist, thus reducing the risk of misclassification.
However, the current study also has limitations. Smoking and obesity could not be taken into account in the overall analysis, because such data were not available for the entire population, but adjustments were made for comorbidities and socioeconomic status. Data from the MBR provided information on smoking and obesity for a subgroup of women, and adjustment for smoking and BMI did not change the overall estimates. Moreover, there are limitations in the method of selecting controls, because there was no data from primary care. Patients with AD diagnosed by general practitioners or who were not even seeking healthcare may have been misclassified as controls. Surveillance bias is a possible cause of differential misclassification. Patients with AD visiting a doctor primarily for other problems are more likely to be diagnosed with AD at the same visit.
The classification of disease severity in the current study has not been validated. AD receiving systemic treatment was defined as severe AD, which has been used as a proxy for disease severity in previous studies (7, 23). In addition, treatment in dermatological wards with AD as the main diagnosis was included as severe AD. Misclassification of disease severity in the current study cannot be excluded if comorbidities were an indication for treatment in dermatological wards or if AD was not the main indication for systemic treatment. Outpatient diagnosis of AD was registered from 2001. Patients with a diagnosis of AD before 2001 could be identified only in the inpatient registry, which is a limitation. This most likely explains why cases of severe AD were older than the non-severe cases in this study. Therefore, comparisons in comorbidity should be made between cases and age-matched controls (Table II) and not between severe and non-severe cases.
Furthermore, we could not adjust for eczema activity over time or take into account the temporal relationship between AD and CVD. AD usually has an onset in early childhood (1, 26); therefore, a reasonable assumption is that the exposure to AD was earlier than onset of CVD in the majority of cases.
An association was found between AD at age 15 years or later and CVD, which remained after multivariable adjustment for known risk factors, such as comorbidities and socioeconomic factors. In conclusion, AD was associated with CVD, which should be kept in mind, especially when managing patients with severe AD. However, definite proof of whether AD is an independent risk factor for CVD requires further confirmation in future prospective trials in which important lifestyle data, such as smoking, are included as possible confounders.
This study was supported by funding from The Swedish Asthma and Allergy Association Research Foundation and the Welander-Finsen Foundation.


 Click to show fullsize
Click to show fullsize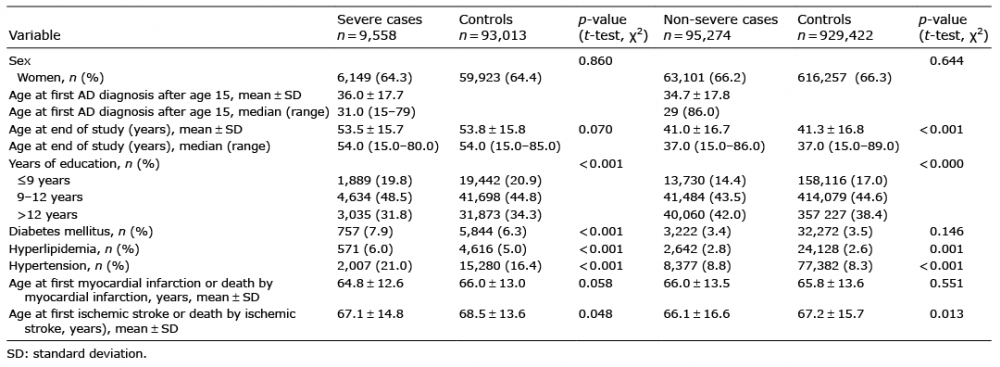 Click to show fullsize
Click to show fullsize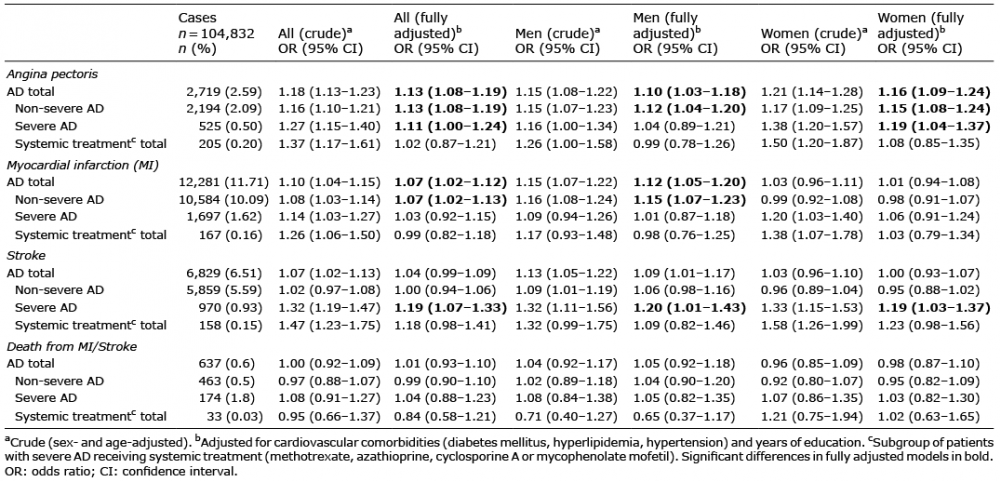 Click to show fullsize
Click to show fullsize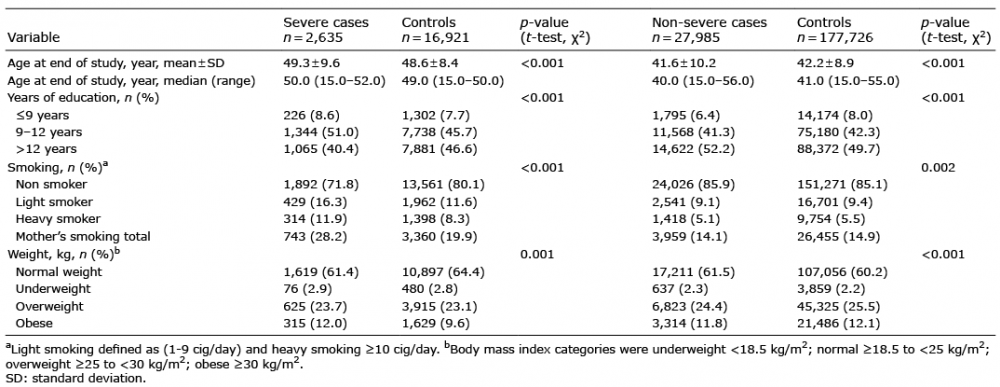 Click to show fullsize
Click to show fullsize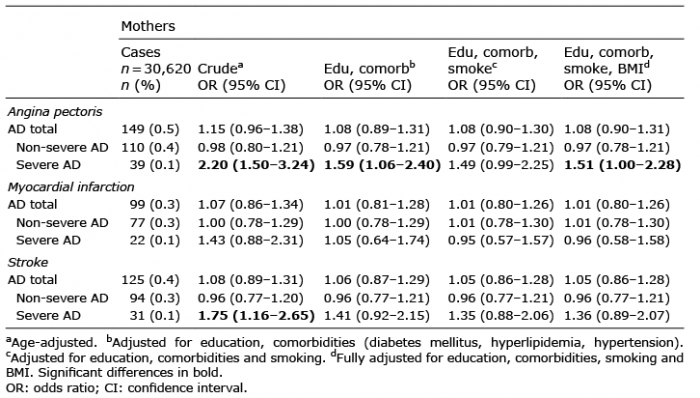 Click to show fullsize
Click to show fullsize